Abstract
The gait is the most complicated, habitual, and involuntary activity of humans and is a result of the cooperation of the central and peripheral nervous systems that harmoniously mobilize the sensory receptors, nervous system, and muscles. A sensory signal binds to a somatosensory system proprioceptor to obtain information on posture. This study was designed to analyze the change in the characteristics of a gait when stimulation is applied in the somatosensory system that controls the balance of the body. A result of the GRF obtained from the force plate and gyroscope signals from the sensor attached on ankle joint were obtained to compare the change before and after the somatosensory stimulation. The result of this study proved a potential of somatosensory stimulation in improving balance, which could be used in studies on the balance of positions and gait improvement.
1. Introduction
The gait is the complicated, habitual, and involuntary activity of humans that involves harmonious movement of 206 bones, hundreds of somatosensory receptors, thousands of nerves, and 636 muscles as a result of the cooperation of the central and peripheral nerve systems. Humans can move the center of their body forward with this continuous movement of their muscles and joints in their lower limbs. The cycles of a gait involve a continuous movement pattern and control the muscles of the trunk, hip joint, knee joint, and feet to maintain the body posture and to enable the person to move forward [1].
During a gait, the human body maintains balance through the various information continuously received from the surroundings and the person’s own body, and responds accordingly. The body organs that are responsible for this aforementioned function are the somatosensory system, the visual system, and the vestibular system. The somatosensory system refers to the deep sensation detected by a proprioceptor in the skin and muscles. The location of each body part, and the posture and movement of the body, can be detected even when a person keeps his eyes closed. This deep sensation or muscle sensation corresponds to the surface sensation. To obtain information on the posture from the signals received in the somatosensory system, the sensory signals should bind accurately to the proprioceptor. Proprioceptors and tactile sensations play essential roles in the maintenance and development of the balance control posture [2].
The peripheral vestibular system quantitatively detects physical forces such as rotation and linear accelerated motion of the head or gravity, transfers the information to electrical signals, and delivers it to the central nervous system. The central nervous system identifies the speed of the head movement and the location of the head in space. With the information on the body location and movement received from the somatosensory organ and visual systems, the central nervous system keeps the body balanced. The vestibular system provides information on head movement and the locations of body parts in relation to gravity and inertial force, and to gravity-inertial frames regarding posture control [3]. The central nervous system combines all the information received from the peripheral vestibular system and other sensory organs (the visual system and the proprioceptors) to identify the location of the head and the movement, and to send orders to the sub-organs after mediating the received information.
Aging and diseases weaken the senses required for posture control, due to which wrong information may be put in this posture control system of our body. The muscular system also begins to lose its ability to stabilize posture when the body posture is unstable [4].
The previous study investigated the correlations between posture stability and the somatosensory system that was stimulated using electrical stimuli, and reported that the swaying gait improved [5]. Another study applied electrical stimulation on the bilateral gastrocnemius muscles and proved its effect on the stability of the static standing position [6]. However, these electrical stimuli have limitations related to stability. A previous study on proprioceptors used a small vibrator to apply stimulation on the eyes, neck, and muscles of the ankle for the investigation of the contribution of the proprioceptive input in the control of the static standing position. The results of the study indicated that the subjects with their eyes closed showed a body swing toward the direction of the muscle swing from the stimulation of the eye muscle, and that the body swing also occurred with the vibration of the sternocleidomastoid and soleus muscles [7]. Another study reported that vibratory stimulation of the soles reduced the variability of the gait of elderly subjects and reduced their risk of falls [8].
A study is needed to analyze the characteristics of the gait of subjects with vestibular system disorder and of elderly subjects who have a weak sensory system when vibratory stimuli are applied to the sensory receptors of their ankle joint during a normal gait. Gait analysis makes use of a specific event or variables being taken place in gait cycle such as division of stance period and swing period of both legs, gait space and time. Therefore, accurately detecting this specific event or variables is essential for researching gait [9]. In the preceding study, objective gait analysis was performed by utilizing extracted gait parameters through gait analysis of 3D motion kinematics utilizing motion analysis system [10-11], that of motor mechanics by using force platform [12], dynamic electromyography (EMG) analysis [13] and plantar pressure analysis [14]. But as these gait analyses could be performed only in a certain space where experiment facility is furnished, there was a spatial limitation and also there was a limitation in natural gait analysis as change of gait pattern was induced [15].
This study was designed to analyze the characteristics of a gait when somatosensory stimulation related to the body surface is used. This study was conducted to supplement the study of the mechanism of the improvement of the senses and the gait of elderly people through somatosensory stimulation. The signals from gyroscope sensors and a force plate during gaits with somatosensory stimulation were extracted and analyzed.
2. Method
This study was conducted to investigate the potential of somatosensory vibratory stimulation to control balance and improve the gait. The following setting was used, and the results were analyzed.
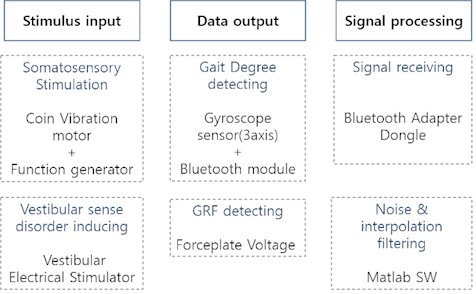
Fig. 1 shows a diagram of the overall system. And Fig. 2 shows the measurement of the system used for the vibratory stimulation and the gait analysis measurement. The system had a gyroscope sensor (three-axis) and a force plate to measure gaits, and a coin vibration motor for applying the vibratory stimulation. An electrical stimulator was used to induce vestibular sense disorder. The measured signals were received as gyroscope signals through a Bluetooth adapter dongle, and the signals from the force plate connected to cables were received and filtered on the main computer.
2.1. Setting of the somatosensory stimuli application
Among the many somatosensors that detect stimuli on the body surface, a mechanoreceptor that detects compression, force, and vibration was required in this study. The Pacinian corpuscle, a receptor that rapidly and significantly responds to vibratory stimuli, was targeted for the stimulation. It is most sensitive in the tendon and at frequencies of 200-300 Hz.
A stimulus with a 250 Hz frequency was applied to the Tibialis Anterior Tendon (TAT) to stimulate the proprioceptors in the tibialis anterior, the muscle in charge of the extension of the ankle muscles. The scale of the vibration differed across the subject based on their individual thresholds, and the threshold value was used when the somatosensory stimulation was applied. For the vibration motor, a linear vibration motor and a foot switch were prepared and attached to the dominant foot of the subjects for the somatosensory stimulation of the TAT.
Fig. 1A diagram of the overall system
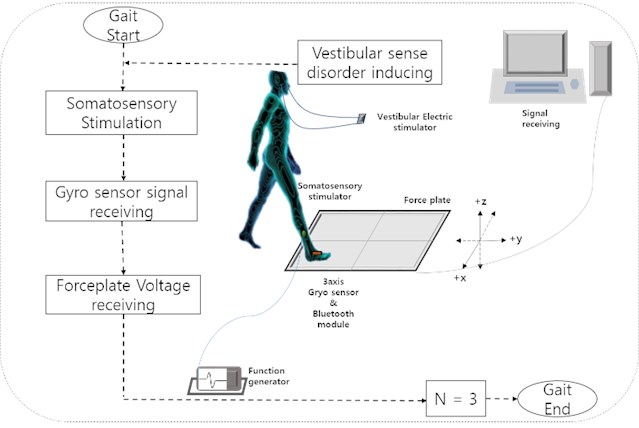
Fig. 2A measurement system used for the stimulation and gait analysis
2.2. Subjects and condition setting for the gait test
Five elderly subjects (age: 68.4±3.66 year, height: 164.74±3.5 cm, weight: 64.5±2.5 kg) who had no neurological disease or abnormality in their vestibular system, had normal musculoskeletal functions, and could walk independently were enrolled in this study. They were all asked to perform a gait with their eyes on the footpath under all the test conditions. They were given a break between the tests that was long enough to relieve any feeling of tiredness they had in their lower limbs, with different stimulation settings. The procedures of the tests were sufficiently explained to them, and their consent was obtained before the test.
The subjects were asked to walk three times when the somatosensory stimulation was applied on the TAT, and another three times when the stimulation was not applied. To analyze the balance of the position during the gait, among the tests of vestibular system abnormality, an additional test was performed three times with the same setting. A gait test was performed for the conditions either with or without abnormality in the vestibular system.
An Ag/AgCL electrode was attached to both mastoid processes to induce abnormality of the vestibular system, and a 0.1 mA Sine wave was applied. The physical theory of the fluctuation-induced maximum frequency of 1 Hz in previous studies was also applied. The abnormality in the vestibular system induced a biased or abnormal gait pattern.
2.3. Detection and analysis of the GRF signal and the gyroscope signals
Gyroscope signals, among the signals that can be detected with small sensors, were used in this study to quantitatively detect the dynamic states of the gaits and to analyze the gait characteristics. An EBIMU-9DOF (E2BOX company, Korea) sensor module that consisted of a three-axis gyroscope, a three-axis accelerator, a three-axis geomagnetic sensor, a 32-bit MCU, and a Parani-ESD200 (Sena Technologies, Inc., Korea) Bluetooth wireless module was used. The gyroscope sensor detected the angular velocity of the Euler angle, which refers to how much the object moved within a certain time, by rotating around each axis. This sensor was attached to the top of the foot with vibratory stimulation, and the signals were detected during the gait test.
The ground reaction force (GRF) is a factor that minimizes energy consumption and is used to evaluate the stability and balance control results. To measure the GRF, four force plates (Bertec Co., U.S.A.) that were embedded in the footpath for the test were used. The sampling frequency was set at 1,000 Hz to be able to detect the change in the location of the supporting foot. The three-axis (, , and ) force and the electrical signals of the moment were detected when a force was loaded on the force plate. These signals passed through the amplifier and the AD converter, and the electrical signals of the analogue output were obtained and used to change the GRF. The GRF was filtered using a MATLAB R2013B program (Mathwork Inc., U.S.A.) divided by the BW (body weight) for standardization.
3. Result
3.1. Gyroscope signal analysis with somatosensory stimulation
For the data extraction factor of the gyroscope signal, the sagittal rotation angle, where plantarflexion and dorsiflexion occur, was extracted and analyzed.
Fig. 3 shows the results of an experiment with five people in which the rotation degree values of the gyroscope signal when a gait was performed without abnormality of the vestibular senses. Fig. 4 shows the results of an experiment with five people in which the rotation degree values of the gyroscope signal when a gait was performed after abnormality of the vestibular senses was induced. As seen in the figures, Initial-Contact (IC) is the moment when a foot touches the ground, and was found to be a characteristic event of a gait that determines the lading response pattern. Toe-off (TO) is the moment when the toes are lifted from the ground and when the rotation angle increases. At that point, Pre Swing (PS) occurs. From IC to TO, a foot that goes through the stance stage performs dorsiflexion and plantarflexion.
Table 1 shows the mean difference in the period and angle between the IC and TO of each subject when he/she performed a gait without vestibular sense abnormality.
The period from the IC to TO decreased when the somatosensory stimulation was applied, unlike when it was not. The rotation angle from the IC to TO increased when the somatosensory stimulation was applied, unlike when it was not. Standard deviation was large, it can be known that a change of the walking is not constant depending on the subject. Table 2 shows the mean difference in the period and angle between the IC and TO of each subject when the gait was performed with abnormal vestibular sense. The period from IC to TO decreased when the somatosensory stimulation was applied, unlike when it was not. Similarly, the rotation angle from the IC to TO increased when the somatosensory stimulation was applied, unlike when it was not. Standard deviation was large, it can be known that a change of the walking is not constant depending on the subject.
Fig. 3Gyro signal during normal gait
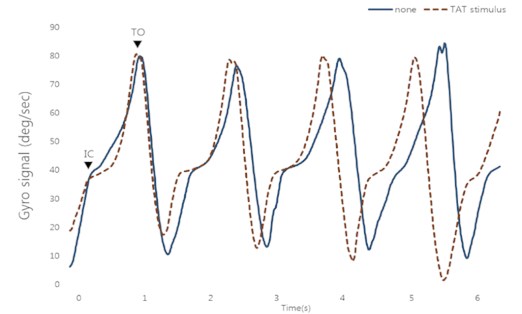
Fig. 4Gyro signal during vestibular sense disorder gait
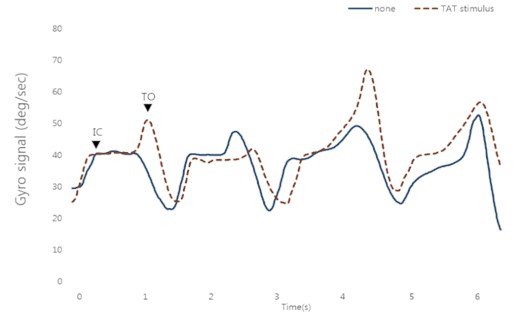
Table 1Gyro signal between IC and TO event during normal gait [means; (SD)]
Time (sec) | Angular (degree) | ||||
None | TAT stimulus | None | TAT stimulus | ||
Difference between IC and TO | Subject 1 | 0.67 (0.19) | 0.66 (0.11) | 35.19 (1.25) | 35.6 (0.82) |
Subject 2 | 0.63 (0.25) | 0.61 (0.09) | 34.26 (3.92) | 38.9 (2.59) | |
Subject 3 | 0.78 (0.17) | 0.68 (0.18) | 37.08 (2.14) | 41.69 (1.39) | |
Subject 4 | 0.66 (0.19) | 0.65 (0.31) | 42.42 (1.82) | 44.44 (0.14) | |
Subject 5 | 0.68 (0.11) | 0.68 (0.29) | 40.3 (0.73) | 41 (3.52) | |
Table 2Gyro signal between IC and TO event during vestibular sense disorder gait [means; (SD)]
Time (sec) | Angular (degree) | ||||
None | TAT stimulus | none | TAT stimulus | ||
Difference between IC and TO | Subject 1 | 0.77 (0.14) | 0.75 (0.21) | 18.91 (2.41) | 20.50 (5.15) |
Subject 2 | 0.86 (0.22) | 0.82 (0.15) | 18.17 (1.56) | 20.11 (3.21) | |
Subject 3 | 0.93 (0.15) | 0.84 (0.17) | 14.15 (0.81) | 15.15 (2.01) | |
Subject 4 | 0.77 (0.17) | 0.82 (0.23) | 21.64 (1.50) | 24.7 (2.09) | |
Subject 5 | 0.75 (0.15) | 0.74 (0.15) | 15.74 (1.11) | 16.12 (0.99) | |
3.2. GRF of the force plate analysis somatosensory with the vibration stimulus application
Fig. 5 shows the results of an experiment with five people in which the vertical GRF of the force plate signals was divided by the weight and standardized when a gait was performed without vestibular sense abnormality. Fig. 6 shows the results of an experiment with five people in which the vertical GRF of the force plate signals were divided by the weight and standardized when a gait was performed after abnormal vestibular sense was induced. As seen in the figures, the vertical GRF had two peaks: the Loading-Response (LR) peak, the initial peak, and the Mid Stance valley between the LR peak and the terminal stance peak. At the LR peak, dorsiflexion occurs and has the biggest GRF value among the LR events. During the LR event that comes after Mid-Stance (MS), weight is received by the foot. The center of gravity falls dramatically and assumes the position that is affected by acceleration. The MS valley appears when the center of gravity in the body rises when the feet are fixed and the body bends forward. This event is affected by the momentum during the swing.
Fig. 5Vertical GRF during normal gait
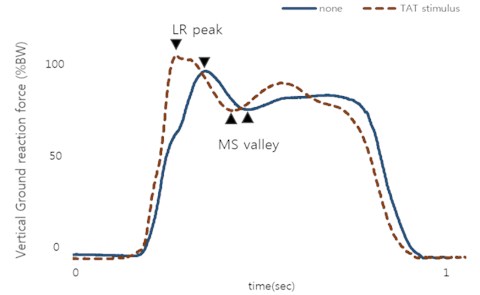
Fig. 6Vertical GRF during vestibular sense disorder gait
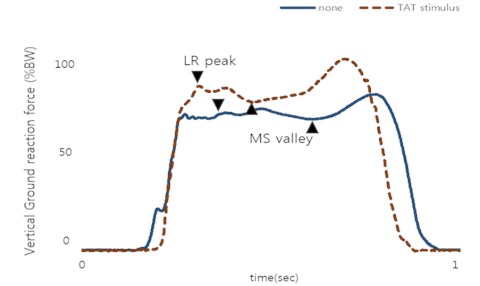
Table 3 shows the mean standardized GRF of the LR peak and the MS valley, and the mean duration of the LR and MS when a gait was performed without vestibular sense abnormality.
The LR peak increased when somatosensory stimulation was applied, unlike when it was not, and the GRF of the MS valley did show a significant difference. The LR and MS periods significantly decreased when somatosensory stimulation was applied, unlike when it was not. It can be known that a change of the walking is not constant depending on the subject. Table 4 shows the mean standardized GRF of the LR peak and the MS valley divided by the weight of each individual subject and the mean period of the LR and the MS when a gait was performed that induced vestibular sense abnormality. The LR peak increased when somatosensory stimulation was applied, unlike when it was not, and the GRF of the MS valley did show a significant difference. The LR and MS periods significantly decreased when somatosensory stimulation was applied, unlike when it was not. It can be known that a change of the walking is not constant depending on the subject.
Table 3Vertical GRF both LR and MS phase during normal gait [means; (SD)]
GRF (BW %) | Time (s) | |||||
None | TAT stimulus | None | TAT stimulus | |||
LR peak | Subject 1 | 105.02 (3.42) | 103.12 (6.42) | LR | 0.171 (0.06) | 0.163 (0.01) |
Subject 2 | 123.44 (3.45) | 120.81 (2.34) | 0.191 (0.06) | 0.170 (0.08) | ||
Subject 3 | 119.16 (4.22) | 118.34 (2.01) | 0.230 (0.09) | 0.219 (0.01) | ||
Subject 4 | 106.58 (2.32) | 104.84 (1.98) | 0.190 (0.04) | 0.190 (0.04) | ||
Subject 5 | 109.31 (2.36) | 113.14 (3.30) | 0.167 (0.01) | 0.164 (0.03) | ||
MS valley | Subject 1 | 91.43 (3.34) | 90.10 (1.31) | MS | 0.141 (0.07) | 0.135 (0.01) |
Subject 2 | 86.90 (4.12) | 84.20 (1.54) | 0.155 (0.02) | 0.153 (0.09) | ||
Subject 3 | 88.85 (4.12) | 85.28 (1.26) | 0.153 (0.01) | 0.143 (0.04) | ||
Subject 4 | 99.64 (2.32) | 96.17 (2.12) | 0.162 (0.04) | 0.149 (0.02) | ||
Subject 5 | 79.65 (4.10) | 81.21 (1.62) | 0.181 (0.01) | 0.171 (0.06) | ||
Table 4Vertical GRF both LR and MS phase during vestibular sense disorder gait [means; (SD)]
GRF (BW %) | Time (s) | |||||
None | TAT stimulus | None | TAT stimulus | |||
LR peak | Subject 1 | 101.20 (1.25) | 104.51 (3.45) | LR | 0.189 (0.02) | 0.181 (0.05) |
Subject 2 | 115.31 (1.72) | 119.93 (2.05) | 0.193 (0.02) | 0.189 (0.02) | ||
Subject 3 | 114.95 (1.9) | 116.34 (0.89) | 0.231 (0.05) | 0.212 (0.03) | ||
Subject 4 | 104.94 (2.41) | 104.41 (0.23) | 0.209 (0.04) | 0.192 (0.05) | ||
Subject 5 | 109.44 (5.21) | 110.22 (3.52) | 0.179 (0.05) | 0.172 (0.06) | ||
MS valley | Subject 1 | 95.30 (3.41) | 92.84 (2.52) | MS | 0.152 (0.06) | 0.142 (0.03) |
Subject 2 | 85.12 (1.45) | 87.24 (1.21) | 0.161 (0.04) | 0.152 (0.03) | ||
Subject 3 | 90.47 (1.90) | 90.92 (2.23) | 0.169 (0.09) | 0.158 (0.05) | ||
Subject 4 | 98.14 (1.45) | 97.20 (2.10) | 0.173 (0.02) | 0.165 (0.04) | ||
Subject 5 | 84.05 (2.11) | 82.23 (1.26) | 0.182 (0.05) | 0.174 (0.03) | ||
4. Conclusions
This study was conducted to investigate the effects of a person’s gait on changes in his or her body balance when vibratory somatosensory stimulation is applied. The following conclusions were reached. The results of this study indicate that various conditions of vibration on the TAT during a normal and vestibular sense disorder gait showed significant effects on the characteristics of the gait of the elderly.
When a gait was performed without an abnormality in the vestibular sense, which is responsible for balance, the significant change in the rotation angle of the gyro signal was deemed to have implied activation of the muscular system responses according to the somatosensory stimulation. When a gait was performed with abnormality of the vestibular senses, the rotation angle of the gyro signals showed a significant change, unlike when no abnormality was induced. Thus, somatosensory stimulation was considered effective in combining the senses involved in balance.
The change in the vertical GRF extracted from the force plate was also deemed to have implied activation of the muscular system responses when a gait was performed without abnormality of the vestibular senses. When a gait was performed with abnormality of the vestibular senses, the vertical GRF showed a significant change with much shorter LR and MS periods than when no abnormality was induced. Thus, somatosensory stimulation was considered effective in combining the senses involved in balance.
The results of this study can be used in studies on controlling and maintaining balance in relation to somatosensory information with vibratory stimulation application, and as data for experimental verification before their use in the establishment of a treatment system. Finally, these findings show that the contribution of vibration on the lower limbs in daily life is important for the use of somatosensory information processing in regulating postural adjustments in elderly individuals.
References
-
Perry J., Schoneberger B. Gait Analysis: Normal and Pathological Function. Slack Inc., New Jersey, 1992.
-
Hlavacka F., Mergner T., Krizkova M. Control of the body vertical by vestibular and proprioceptive inputs. Brain Research Bulletin, Vol. 40, 1996, p. 431-434.
-
Shumway-Cook A., Woollacott M. H. Motor Control: Theory and Practical Applications. First Edition. Williams and Wilkins Inc., Baltimore, 1995.
-
Robert S. M., Peter C., William J. E., Maria F., James H., Edward M., Jill S. ACSM position stand: exercise and physical activity for older adults. Medicine and Science in Sport and Exercise, Vol. 30, 1998, p. 992-1008.
-
Gracelle D. C., Laughton C. A., Dhruv N. T., Datdare K. D., Niemi J. B., Lipsitz L. A., Collins J. J. Noise-enhanced balance control in older adults. Neuroreport, Vol. 13, Issue 15, 2002, p. 1853-1856.
-
Dickstein R., Laufer Y., Katz M. TENS to the posterior aspect of the legs decreases postural sway during stance. Neuroscience Letters, Vol. 393, 2006, p. 51-55.
-
Ivanenko Y. P., Grasso R., Lacquaniti F. Neck muscle vibration makes walking humans accelerate in the direction of gaze. The Journal of Physiology, Vol. 525, 2000, p. 803-814.
-
Galica A. M., Kand H. G., Priplata A. A., D’Andrea S. E., Starobinets O. V., Sorond F. A., Cupples L. A. and Lipsitz L. A. Subsensory vibrations to the feet reduce gait variability in elderly fallers. Gait and Posture, Vol. 30, 2009, p. 383-387.
-
Rueterbories J., Spaich E. G., Larsen B., Andersen O. K. Methods for gait event detection and analysis in ambulatory systems. Medical Engineering and Physics, Vol. 32, Issue 6, 2010, p. 545-552.
-
O’Connor C. M., Thorpe S. K., O’Malley M. J., Vaughan C. L. Automatic detection of gait events using kinematic data. Gait and Posture, Vol. 25, Issue 3, 2004, p. 469-474.
-
Hreljac A., Marshall R. N. Algorithms to determine event timing during normal walking using kinematic data. Journal of Biomechanics, Vol. 33, Issue 6, 2000, p. 783-786.
-
Muniz A. M. S., Nadal J., Application of principal component analysis in vertical ground reaction force to discriminate normal and abnormal gait. Gait and Posture, Vol. 29, Issue 1, 2009, p. 31-35.
-
Stolzea H., Kuhtz-Buschbecka J. P., Mondwurfa C., Boczek-Funckea A., Johnka K., Deuschlb G., Illert M. Gait analysis during treadmill and overground locomotion in children and adults. Electroencephalography and Clinical Neurophysiology/Electromyography and Motor Control, Vol. 105, Issue 6, 1997, p. 490-497.
-
Hayafune N., Hayafune Y., Jacob H. A. C. Pressure and force distribution characteristics under the normal foot during the push-off phase in gait. The Foot, Vol. 9, Issue 2, 1999, p. 88-92.
-
Parvataneni K., Ploeg L., Olney S. J., Brouwer B. Kinematic, kinetic and metabolic parameters of treadmill versus overground walking in healthy older adults. Clinical Biomechanics, Vol. 24, Issue 1, 2009, p. 95-100.
About this article
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIP) (NRF-2014R1A2A1A11053073).
